Lower-Limb Amputee Rehabilitation
Transtibial deviations
Stance deviations in transtibial amputees.
(Murphy, 2013; Spires, Kelly & Davis, 2013; Nelson et al., 2006)
Deviations
Amputee causes
Prosthesis causes
Example
Foot slap
Foot progresses too quickly from heel contact to flat foot on prosthetic side, creating a slapping sound
Decreased eccentric quadriceps control
Decreased confidence
Worn out or too soft heel
Excessive socket flexion
Excessive dorsiflexion
Foot rotation at IC
External rotation of prosthetic foot at initial contact
Poor muscle control of residual limb
Pain
Extension of residual limb is too vigorous at IC
Plantarflexion bumper too stiff
Heel wedge too hard
Poor suspension allowing for rotation
Insufficient socks
Too much toe-out in prosthetic alignment
Knee extension/
hyperextension
Excessive extension of knee in stance
As body moves over the limb in terminal stance, the ground reaction force moves anterior to the knee joint. If this moment is too large, excessive knee extension is seen
Weak quadriceps
Gastrocnemius weakness
Genu recurvatum
Ligamentous laxity
Knee joint instability
Poor hip/knee coordination
Socket in extension/posterior tilt
Too soft heel bumper
Excessive foot plantarflexion
Heel height of shoe too low (usually if patient changes shoes after being fitted with prosthesis)
Decreased push off
Insufficient push off in terminal stance to pre-swing on prosthetic side
Fear of placing entire weight on prosthesis
Loss of power due to the loss of tissue at the gastroc-soleus complex across the ankle joint
Foot too dorsiflexed
Foot too posterior, causing a shortened anterior lever arm
Excessive knee flexion
Excessive knee flexion greater than 10 degrees throughout stance
Knee flexion contracture
Hip flexion contracture
Weak inner range quadriceps
Weak glutes
Pain
Socket in flexion/anterior tilt
Socket set too far forward
Foot too dorsiflexed
Excessively stiff plantarflexion bumper or heel cushion
Poor suspension
Walking on medial
border of foot
Excessive weight or time spent on inner/medial border of foot (varus gait)
Decreased hip musculature control
Genu valgum
Prosthesis too adducted
Foot too outset
Uneven wear of shoe heel
Walking on lateral
border of foot
Excessive weight or time spent on outer/lateral border of foot (valgus gait)
Genu varum
Prosthesis too abducted
Prosthetic foot too inset
Uneven wear of shoe heel
Narrow base of support
Decreased horizontal distance between heels during double support
Weak hip abductors
Hip adductor contracture
Decreased proprioception
Genu varum
Socket too abducted
Prosthetic foot too far inset
Wide base of support
Increased horizontal distance between heels during double support (abducted gait)
Hip abductor contracture or spasticity
Genu valgum
Compensation for instability
Prosthesis too long
Prosthetic foot too outset
Excessive heel rise
Prosthetic heel rising excessively and rapidly when knee is flexed at the beginning of swing phase
Decreased glute strength
Decreased quads control
Pain
Hip or knee flexion contracture
Compensation to assist in toe clearance
Excessive foot dorsiflexion
Socket set too posterior
Excessive socket flexion
Foot set too posterior
Medial whip
Heel of prosthetic foot moves medially at toe off
Typically less pronounced than with TFA
Severe muscle strength and/or length imbalance
Incorrectly donned socket
Prosthetic foot alignment
Swing deviations in transtibial amputees.
(Murphy, 2013; Spires, Kelly & Davis, 2013; Nelson et al., 2006)
Deviations
Amputee causes
Prosthesis causes
Image or Video example
Trendelenburg gait
Lateral lean over weight bearing limb
Hip abductor weakness
Stump pain
Hip pain
Poor balance
Poor confidence
Short prosthesis
Functionally short prosthesis, e.g. not wearing enough sock ply
Prosthetic foot set too laterally
Pain from socket
Lateral whip
Heel of prosthetic foot moves laterally at toe off
Severe muscle strength and/or length imbalance
Incorrectly donned socket
Prosthetic foot alignment
Circumduction
Prosthesis swinging in laterally curved arc during swing phase
Hip abduction contracture
Desire to keep knee locked during gait
Weak hip flexors
Weak hamstrings
Poor proprioception
Pain
Prosthesis too long
Prosthesis functionally too long due to loss of suspension, wearing too many socks, or excessively plantarflexed foot
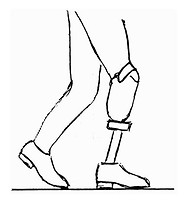
Vaulting
Plantarflexion during midstance on intact limb to clear prosthetic foot while prosthesis moves through swing
Can often accompany circumduction
Desire to keep knee locked during gait
Poor gait habit developed from previously using a prosthesis that was too long
Prosthesis too long
Dorsiflexion bumper too soft
Compensatory mechanism to clear prosthetic foot during swing due to long or functionally long prosthesis
References:
Corewalking (2017). Trendelenburg gait. Retrieved from: https://corewalking.com/trendelenburg-gait/
Morgan, C. (2012). Hip flexion contracture reasons. Retrieved from: http://sharonkaram.com/tag/flexion/page/5/
Murphy, D. (2013). Fundamentals of Amputation Care and Prosthetics. New York: Demos Medical Publishing.
Nelson, V. S., Flood, K. M., Bryant, P. R., Huang, M. E., Pasquina, P. F., & Roberts, T. L. (2006). Limb deficiency and prosthetic management. 1. Decision making in prosthetic prescription and management. Archives of physical medicine and rehabilitation, 87(3), 3-9. doi: 10.1016/j.apmr.2005.11.022
pdhpe (2015). Base of support. Retrieved from: https://www.pdhpe.net/the-body-in-motion/how-do-biomechanical-principles-influence-movement/balance-and-stability/base-of-support/
Spires, M. C., Kelly, B., & Davis, A. (2013). Prosthetic restoration and rehabilitation of the upper and lower extremity. New York: Demos Medical Publishing

Narrow base of support (pdhpe, 2015)

Wide base of support (pdhpe, 2015)
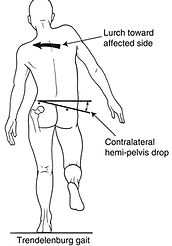
Trendelenburg gait (Corewalking, 2017)
Knee flexion in stance (Morgan, 2012)